Shoulder Dislocation: What You Need to Know for a Safe and Strong Recovery
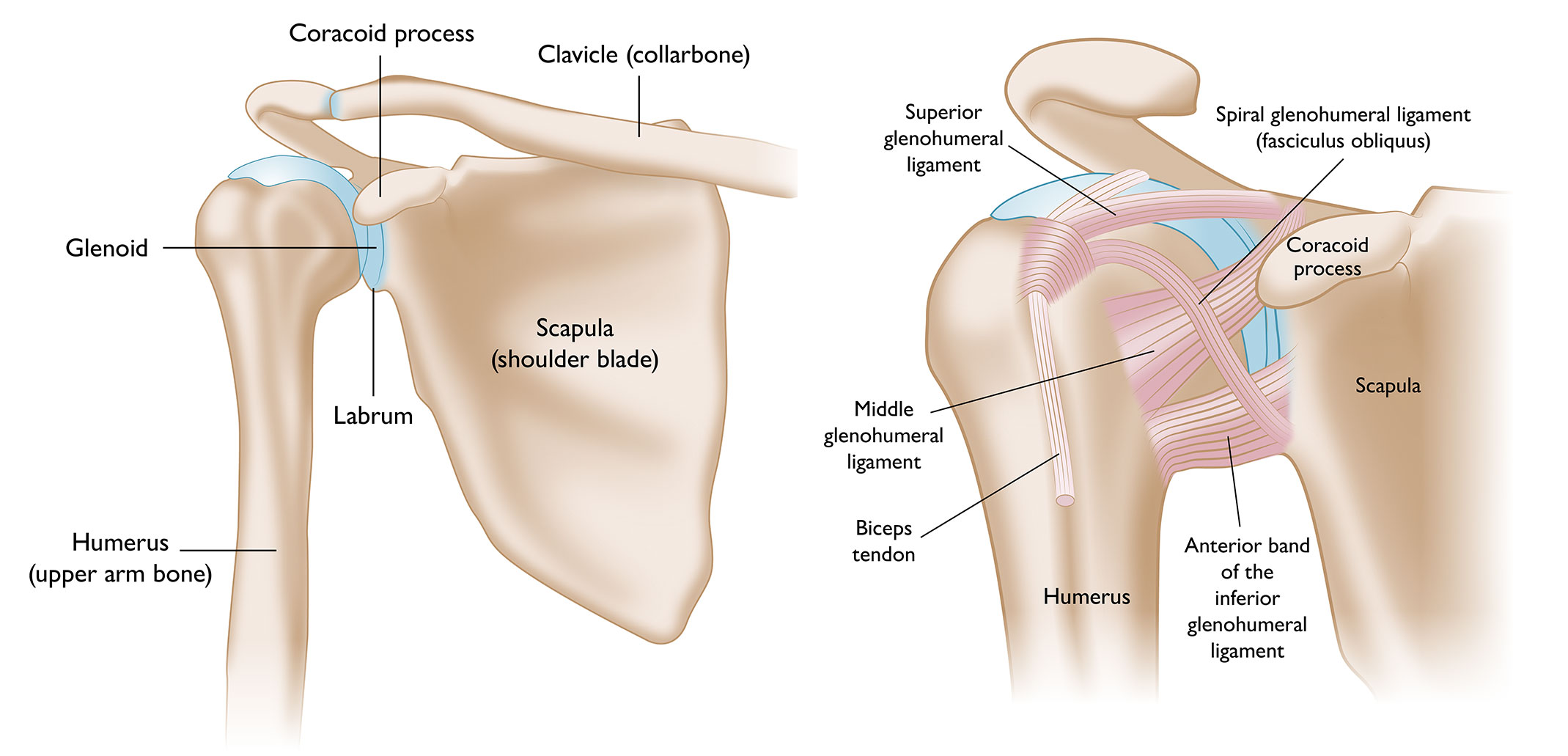
A shoulder dislocation is one of the most painful and destabilizing orthopedic injuries you can experience. When the humeral head is forced out of the glenoid socket, it doesn’t just disrupt joint alignment—it stretches or tears surrounding ligaments, damages the labrum, and resets your neuromuscular control.
But here’s the good news: with a structured, evidence-based approach to shoulder dislocation recovery, most people regain full function, strength, and confidence. Whether you’re navigating your first dislocation or managing recurrent instability, this guide breaks down exactly what to do, what to avoid, and how to rebuild a resilient shoulder for the long term.
Shoulder Dislocation: More Than Just a “Popped Out” Joint
The shoulder is the most mobile joint in the human body, which also makes it the most prone to dislocation. In over 90% of cases, the humeral head slips forward (anterior dislocation), often from a fall, sports collision, or sudden overhead force. Less commonly, it dislocates posteriorly or inferiorly.
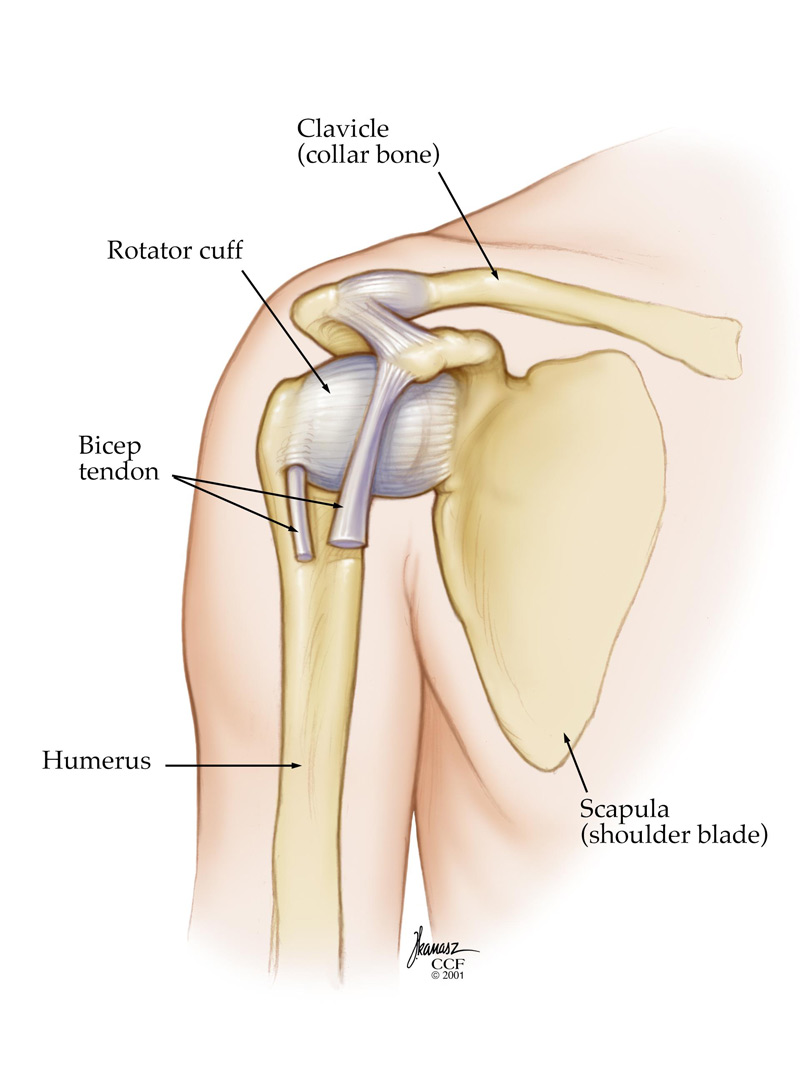
What many patients don’t realize is that the initial injury is only the beginning. The surrounding structures—the labrum, rotator cuff tendons, joint capsule, and proprioceptive nerve endings—are often compromised. Without proper rehabilitation, this can lead to chronic shoulder instability, recurrent dislocations, or early-onset osteoarthritis.
A successful shoulder dislocation recovery hinges on three pillars:
- Tissue healing (ligaments, labrum, capsule)
- Neuromuscular re-education (restoring joint position sense and dynamic stability)
- Progressive load management (strengthening without re-injury)
Immediate Steps After a Shoulder Dislocation (What to Do First)
Knowing what to do after shoulder dislocation can significantly impact your long-term outcome. In the acute phase (first 48–72 hours), focus on:
- Medical reduction: Never attempt to “pop it back in” yourself. Improper manipulation can fracture the humerus or damage nerves (especially the axillary nerve).
- Immobilization: A sling or shoulder immobilizer protects healing tissues. Current protocols favor shorter immobilization periods (3–7 days for first-time dislocations) to prevent stiffness.
- Ice & elevation: Apply ice for 15–20 minutes every 2–3 hours to reduce swelling and pain.
- Pain management: NSAIDs or prescribed medications can control inflammation, but consult your provider before long-term use, as excessive anti-inflammatory use may interfere with early tissue repair.
- Imaging & diagnosis: X-rays confirm reduction and rule out fractures. An MRI or MR arthrogram is often recommended to assess labral tears (like Bankart or Hill-Sachs lesions), which heavily influence recovery pathways.
The Phased Recovery Timeline for a Dislocated Shoulder
How long does a dislocated shoulder take to heal? The answer depends on age, activity level, severity of soft tissue damage, and whether surgery was required. However, a standard non-surgical timeline follows four progressive phases. Rushing ahead of tissue readiness is the #1 cause of setbacks.
Phase 1: Protection & Pain Management (Weeks 0–2)
- Goal: Control inflammation, protect healing structures, prevent muscle atrophy
- Focus: Sling use as directed, pendulum exercises, scapular retraction drills, gentle wrist/elbow mobility
- Avoid: Lifting, overhead reaching, external rotation under load
- NLP Note: Early mobilization within pain-free ranges stimulates collagen alignment and reduces adhesive capsulitis risk.
Phase 2: Restoring Range of Motion (Weeks 2–6)
- Goal: Regain full, pain-free joint mobility
- Focus: Passive and active-assisted ROM exercises, pulley systems, wall slides, sleeper stretches (if cleared)
- Physical therapy for shoulder dislocation typically introduces light isometric contractions here to activate stabilizers without joint shear.
- Milestone: Full forward flexion and external rotation matching the uninjured side (within 10–15°).
Phase 3: Strengthening & Stability (Weeks 6–12)
- Goal: Rebuild rotator cuff endurance, scapulothoracic control, and dynamic joint stability
- Focus: Resistance band external/internal rotation, prone Y/T/W raises, closed-chain weight shifts, proprioceptive ball drills
- Shoulder dislocation rehab exercises now emphasize neuromuscular control: teaching the shoulder to stabilize under light load before progressing to heavy resistance.
- Milestone: 80–90% strength symmetry, pain-free daily function, stable overhead positioning.
Phase 4: Return to Activity & Sport-Specific Training (Months 3–6+)
- Goal: Prepare for work, sport, or high-demand activities
- Focus: Plyometrics, deceleration training, sport-specific drills, gradual load progression
- Clearance criteria: Full ROM, strength ≥90% of contralateral side, negative apprehension/relocation tests, successful completion of functional movement screen.
- Note: Contact athletes often require 4–6 months; overhead athletes (swimmers, pitchers, tennis players) may need 6–9 months for full biomechanical restoration.
Surgical vs. Non-Surgical Recovery: Which Path Is Right for You?
Not every dislocation requires surgery, but certain factors tilt the scale toward operative intervention:
| Non-Surgical Recovery | Surgical Recovery (Arthroscopic Stabilization) |
| First-time dislocation, age >30 | Age <25, high recurrence risk (up to 70–90% without surgery) |
| Minimal labral/capsular damage | Significant Bankart tear, Hill-Sachs lesion, or bone loss |
| Low-demand lifestyle or non-contact sport | Contact/overhead athlete, labor-intensive occupation |
| Timeline: 3–4 months to full function | Timeline: 4–6 months sling modification, 6–9+ months full return |
Recurrent shoulder dislocation treatment often involves arthroscopic labral repair and capsular plication. Post-op rehab is more structured, with strict ROM restrictions for the first 4–6 weeks to protect suture anchors. However, long-term stability rates exceed 90% when rehab compliance is high.
Common Mistakes That Delay Shoulder Dislocation Recovery
Even with the best medical guidance, patients unknowingly sabotage their progress. Avoid these pitfalls:
- Removing the sling too early: Premature stress stretches healing ligaments before collagen matures.
- Skipping scapular work: The shoulder blade is the foundation of glenohumeral stability. Weak serratus anterior or lower traps force the rotator cuff to overcompensate.
- Overloading external rotation too soon: The anterior capsule is most vulnerable in 90° abduction + external rotation. Respect tissue timelines.
- Ignoring proprioception: Joint position sense degrades after dislocation. Without balance and reactive stability drills, the shoulder remains “blind” to sudden loads.
- Comparing timelines: Recovery is nonlinear. Pain-free progression > calendar dates.
Frequently Asked Questions (FAQ)
Q: Can a dislocated shoulder heal without physical therapy?
A: While mild cases may recover with rest and home exercises, structured physical therapy for shoulder dislocation significantly reduces recurrence risk. PT restores neuromuscular control, addresses compensatory movement patterns, and safely progresses load—something generic routines often miss.
Q: How long does a dislocated shoulder take to heal completely?
A: Soft tissue healing takes 6–12 weeks, but full functional recovery typically requires 3–6 months. Athletes or those with labral repairs may need 6–9 months. Healing isn’t just about pain resolution; it’s about restoring dynamic stability under load.
Q: What are the best shoulder dislocation rehab exercises for home?
A: Early-stage safe options include pendulum swings, scapular retractions, isometric external/internal rotation against a wall, and resistance band rows. Always progress under professional guidance to avoid impingement or instability.
Q: When should I consider surgery for recurrent shoulder dislocation treatment?
A: If you experience two or more dislocations, feel persistent “slipping” or apprehension, or participate in contact/overhead sports, surgical stabilization is often recommended. Early intervention prevents cartilage wear and chronic instability.
Q: Can I return to weightlifting after a shoulder dislocation?
A: Yes, but with modifications. Avoid extreme external rotation under load (e.g., behind-the-neck presses, wide-grip bench) until cleared. Focus on controlled tempo, scapular control, and rotator cuff endurance before max loading.
Take the Next Step in Your Shoulder Dislocation Recovery
Recovering from a dislocated shoulder isn’t just about waiting for pain to fade—it’s about rebuilding a joint that’s stronger, smarter, and more resilient than before. Whether you’re in week one or month four, the right guidance makes the difference between a full return and a cycle of re-injury.
👉 Don’t navigate recovery alone. Book a personalized shoulder stability assessment with our certified orthopedic physical therapists today. You’ll receive a custom rehab roadmap, video-guided exercise library, and clear milestones to track your progress—backed by clinical evidence and tailored to your sport, job, and lifestyle.
📅 Schedule Your Recovery Consultation Now
Limited new-patient slots available each week. Secure your spot and start moving with confidence again.