Cuff Injury: Symptoms and Risk Factors – A Complete Guide
Quick Answer Summary
Cuff injuries, commonly referring to rotator cuff tears or injuries of the upper extremity cuffs, present as shoulder pain, weakness, and limited range of motion. Risk factors include age (40+ years), repetitive overhead activities, previous shoulder trauma, poor posture, and certain medical conditions. Early diagnosis and treatment at a specialized clinic like NBR Clinic in Lahore under the care of Dr. Riaz Ahmed, a leading sports medicine specialist, can significantly improve outcomes and prevent long-term disability.
1. Introduction to Cuff Injuries
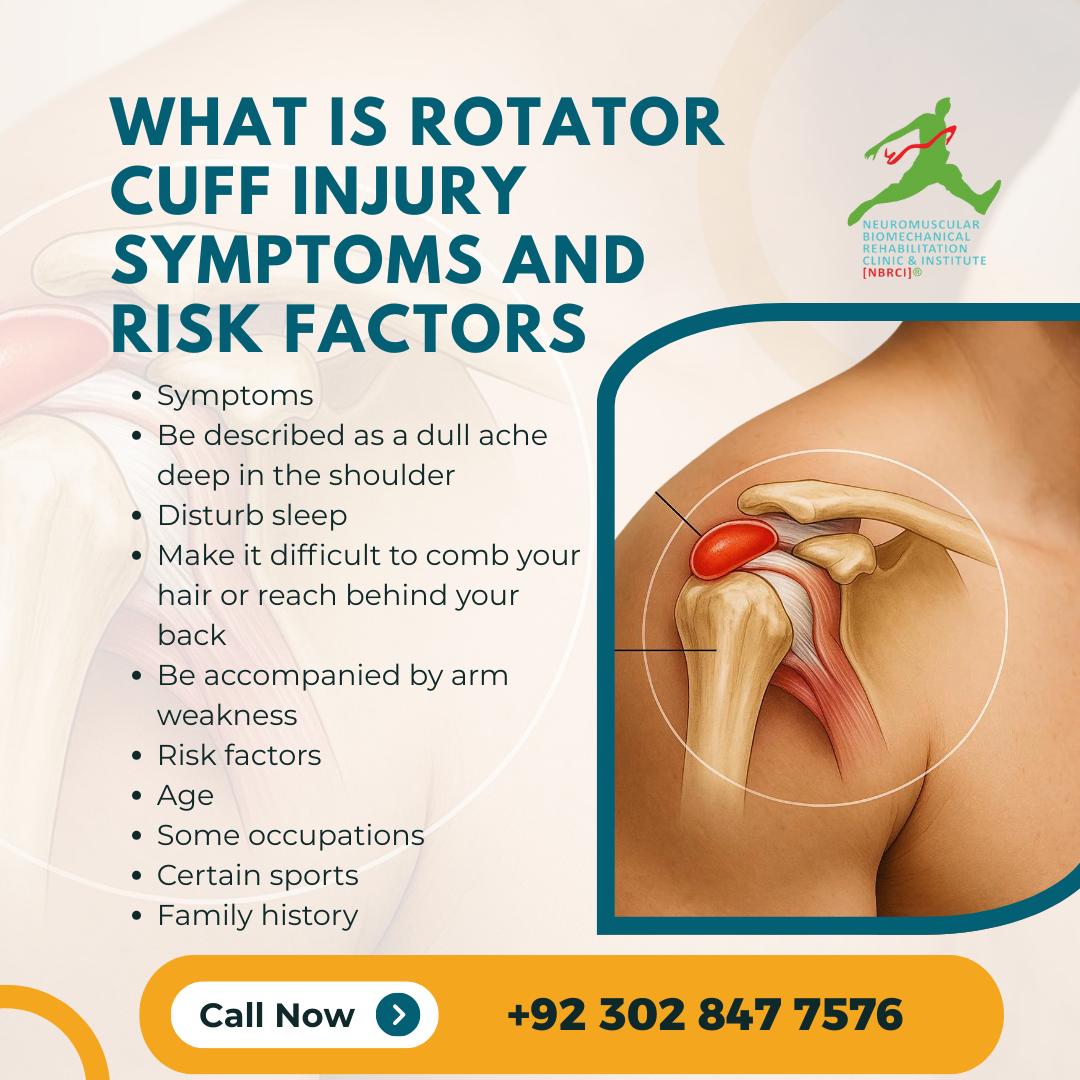
Cuff injuries represent a significant healthcare concern affecting millions of individuals worldwide, with particularly high prevalence in Lahore and across Pakistan’s active population. These injuries typically involve the rotator cuff—a group of muscles and tendons that stabilize and enable movement of the shoulder joint.
The rotator cuff comprises four muscles: the supraspinatus, infraspinatus, teres minor, and subscapularis. When these structures become injured, individuals experience varying degrees of pain, functional limitation, and weakness that can significantly impact daily activities, work performance, and quality of life.
Key entities related to cuff injuries include:
- Rotator cuff muscles (supraspinatus, infraspinatus, teres minor, subscapularis)
- Shoulder joint structures (glenohumeral joint, acromion, humeral head)
- Associated conditions (impingement syndrome, bursitis, tendonitis)
- Associated joints (acromioclavicular joint, sternoclavicular joint)
- Understanding Cuff Anatomy and Function
2.The Rotator Cuff Structure
The rotator cuff is a sophisticated network of muscles and tendons working in concert to:
- Stabilize the shoulder joint during movement
- Enable internal and external rotation
- Support arm elevation and overhead movements
- Maintain proper glenohumeral centration
The supraspinatus muscle initiates arm abduction and is most commonly affected by cuff injuries. The infraspinatus and teres minor facilitate external rotation, while the subscapularis enables internal rotation and provides anterior stability.
Biomechanics and Movement Patterns
Understanding shoulder biomechanics is essential for comprehending how injuries develop. The shoulder joint operates through a complex interaction of:
- Scapular positioning and movement (scapulohumeral rhythm)
- Glenohumeral joint stability
- Neuromuscular control and coordination
- Load distribution across multiple anatomical structures
When biomechanical dysfunction occurs—whether from muscular weakness, postural deviation, or impaired kinematics—the rotator cuff bears excessive stress, leading to microtrauma and eventual injury.
3. Comprehensive Symptoms of Cuff Injuries
Primary Symptoms
Shoulder Pain
Individuals with cuff injuries characteristically experience:
- Localized pain in the anterolateral shoulder region, often worse at night
- Pain with specific movements, particularly overhead activities and cross-body adduction
- Pain during sleep, especially when lying on the affected shoulder
- Gradual onset in degenerative tears versus acute pain in traumatic injuries
The pain often radiates down the arm toward the elbow but rarely extends to the hand, distinguishing it from cervical radiculopathy or neurological conditions.
Weakness and Functional Limitation
Patients frequently report:
- Weakness during arm elevation, particularly at 60-120 degrees of abduction (positive “drop arm test”)
- Difficulty performing overhead activities (reaching for objects, throwing, swimming)
- Reduced ability to perform routine tasks (combing hair, dressing, lifting)
- Progressive functional decline if left untreated
Range of Motion Restrictions
Cuff injuries typically result in:
- Limited active range of motion (patient-initiated movement)
- Preserved passive range of motion (examiner-assisted movement)
- Specific loss of external rotation and abduction
- Secondary stiffness from protective muscular guarding
Secondary Symptoms
Night Pain and Sleep Disturbance
Night pain is highly characteristic of rotator cuff pathology and occurs due to:
- Loss of muscular support during sleep
- Dependent positioning of the arm
- Increased inflammatory activity in the evening
- Psychological amplification of symptoms in quiet environments
Clicking, Popping, or Crepitus
Some patients describe:
- Mechanical symptoms suggesting incomplete tendon tears or internal derangement
- Associated subacromial bursitis causing crepitus
- Sound generation from irregular tendon surfaces
Stiffness and Morning Symptoms
- Morning stiffness lasting 30 minutes to several hours
- Gradual improvement with activity (warm-up phenomenon)
- Return of stiffness after prolonged rest
Referred Pain Patterns
Cuff injuries may produce:
- C5 dermatome pain referral (lateral shoulder and arm)
- Cervical pain referred to the shoulder
- Scapular region discomfort from compensatory muscle tension
4. Risk Factors and Predisposing Conditions
Age-Related Risk Factors
Progressive Degenerative Changes
Risk of cuff injury increases significantly with advancing age:
- 40-50 years: Initial increased prevalence of small tears
- 50-60 years: Rapid acceleration of degenerative changes
- 60+ years: High prevalence of asymptomatic tears (estimates 20-25% of population)
Age-related factors contributing to cuff vulnerability include:
- Decreased cellularity and vascularity of tendon tissue
- Progressive collagen cross-linking and reduced elasticity
- Declining intrinsic muscle strength and motor control
- Reduced growth factor availability and healing capacity
Biomechanical Risk Factors
Postural Dysfunction
Modern lifestyle and occupational patterns create predisposing postural abnormalities:
- Forward head posture (common in office workers using computers)
- Rounded shoulder positioning from desk work
- Scapular dyskinesis (abnormal scapular movement patterns)
- Kyphotic thoracic spine reducing space for rotator cuff
These postural deviations alter glenohumeral mechanics and create subacromial impingement.
Muscle Imbalance and Weakness
Common imbalances increasing cuff injury risk include:
- Weak external rotators relative to internal rotators
- Weak scapular stabilizers (serratus anterior, lower trapezius)
- Tight internal rotators (pectoralis major, subscapularis)
- Weak posterior deltoid and infraspinatus
- Underlying generalized strength deficits
Range of Motion Restrictions
Limited flexibility predisposes to injury:
- Glenohumeral internal rotation deficit (GIRD) from tight posterior capsule
- Restricted external rotation limiting load distribution
- Limited thoracic extension compensated by shoulder extension
- Reduced scapular external rotation
Activity-Related Risk Factors
Overhead Activities
Professions and sports involving repetitive overhead movements carry significantly elevated cuff injury risk:
- Overhead athletes: Throwing sports (baseball, javelin), swimming, tennis, badminton
- Occupational overhead work: Painters, construction workers, electricians
- Gymnastics and weightlifting: Explosive overhead movements under load
- Military personnel: Combat conditioning and equipment handling
Overhead activities create extreme glenohumeral joint positions increasing impingement risk and shear forces.
Repetitive Arm Activities
Sustained repetitive motion increases microtrauma risk:
- Assembly line work with sustained arm positioning
- Typing and computer work in combination with poor posture
- Driving for extended periods with sustained shoulder positioning
- Manual labor requiring sustained force production
Medical and Systemic Risk Factors
Age-Related Degenerative Conditions
- Osteoarthritis of the glenohumeral joint
- Acromioclavicular joint arthropathy (osteophyte formation narrowing subacromial space)
- Calcific tendonitis from calcium phosphate crystal deposition
- Subacromial bursitis from chronic impingement
Metabolic and Systemic Conditions
Certain systemic conditions increase cuff pathology risk:
- Diabetes mellitus: Associated with reduced healing capacity and increased stiffness risk
- Rotator cuff calcification: Often associated with vitamin D deficiency, chronic kidney disease, and other metabolic abnormalities
- Hyperlipidemia: Associated with tendon degeneration
- Thyroid dysfunction: Links to musculoskeletal complications
- Autoimmune conditions: Rheumatoid arthritis, lupus affecting shoulder structures
Psychiatric and Psychological Factors
Emerging evidence suggests psychological factors affect cuff injury outcomes:
- Catastrophizing about injury predicts worse functional outcomes
- Anxiety and depression correlate with pain perception
- Low self-efficacy relates to delayed rehabilitation engagement
- Sleep quality directly impacts healing processes
Traumatic and Injury-Related Risk Factors
Previous Shoulder Injuries
- Previous cuff tears: First tear predicts subsequent tears (recurrence rate 5-30% depending on treatment)
- Shoulder dislocation: Disrupts stabilizing structures, increases long-term cuff injury risk
- Anterior shoulder instability: Alters mechanics, increasing overload on cuff
- Labral tears: Associated capsular laxity affects cuff loading
Acute Traumatic Events
- Falls on outstretched hand creating sudden loading
- Direct blow to shoulder causing acute structural damage
- Massive sudden force during sporting activities
- Motor vehicle accidents with shoulder impact trauma
Lifestyle and Environmental Factors
Smoking
Smoking significantly impairs healing:
- Reduces blood flow to tendon tissue
- Impairs collagen synthesis and cross-linking
- Increases inflammation and oxidative stress
- Associated with treatment failure and higher recurrence rates
Studies demonstrate smokers have 1.5-2 times higher risk of cuff injury and poorer outcomes after treatment.
Sedentary Lifestyle
- Poor cardiovascular conditioning reduces metabolic support for healing
- Reduced muscular endurance capacity for cuff function
- Obesity-related inflammatory state
- Accelerated deconditioning cascade
Occupational and Sport-Specific Demands
In Lahore and surrounding regions, specific occupational and recreational patterns create elevated risk:
- Textile and manufacturing workers with repetitive arm positioning
- Rickshaw and vehicle operators with sustained shoulder positioning
- Construction and carpentry with overhead and forceful activities
- Badminton and cricket players with high-velocity overhead movements
5. Diagnosis and Assessment
Clinical Evaluation
Professional diagnosis begins with comprehensive clinical assessment by specialists like Dr. Riaz Ahmed at NBR Clinic. This includes:
History Taking
- Detailed onset and progression of symptoms
- Mechanism of injury (traumatic versus insidious)
- Activity exacerbation patterns
- Night pain characteristics
- Previous injuries or interventions
- Occupational and recreational activity demands
Physical Examination
Standardized examination tests include:
Supraspinatus Assessment
- Drop Arm Test: Patient holds arm at 90 degrees abduction; inability to lower slowly indicates cuff tear
- Supraspinatus Strength Test: Resistance to abduction in scapular plane (0-90 degrees)
- Jobe’s Crank Test: Abduction with thumb pointing down (“empty can” position)
Infraspinatus and Teres Minor Assessment
- Infraspinatus Strength Test: Resistance to external rotation at 90 degrees abduction
- External Rotation Lag Sign: Inability to maintain external rotation when passive support removed
- Hornblower’s Sign: Inability to maintain external rotation at 0 degrees abduction
Subscapularis Assessment
- Lift-Off Test: Difficulty pressing lower back against wall
- Belly-Press Test: Modified assessment when lift-off impossible
- Internal Rotation Lag Sign: Inability to maintain internal rotation when passive support removed
Comprehensive Shoulder Assessment
- Scapular Dyskinesis Observation: Assessment of scapular movement during abduction
- Posterior Shoulder Tightness: Cross-body adduction test and sleeper stretch assessment
- Glenohumeral Instability Testing: Anterior and posterior drawer tests, load-and-shift test
- Impingement Signs: Neer and Hawkins impingement signs
Imaging and Diagnostic Modalities
Radiographs (X-rays)
Standard radiographs serve as initial imaging and reveal:
- Acromioclavicular joint arthropathy (osteophytes narrowing space)
- Humeral head position (superior migration suggesting massive tear)
- Osseous changes from degenerative disease
- Acromion morphology (hooked vs. flat configurations)
Ultrasound Imaging
Ultrasound offers real-time assessment advantages:
- Excellent soft tissue resolution for tendon evaluation
- Dynamic assessment of muscle and tendon during movement
- Operator and patient-dependent variability
- Sensitivity 68-98% for full-thickness tears depending on tear size and examiner experience
- Cost-effective and readily available at clinics like NBR
Magnetic Resonance Imaging (MRI)
MRI provides detailed structural assessment:
- Superior contrast resolution for soft tissue characterization
- Precise tear size and location measurement
- Associated pathology identification (bursitis, labral tears)
- Fatty infiltration assessment (predicting repair success)
- High sensitivity and specificity (>90% for rotator cuff pathology)
- Higher cost and longer acquisition time
MRI Arthrography
Enhanced MRI with intra-articular contrast reveals:
- Partial-thickness articular-side tears not visible on standard MRI
- Labral pathology with enhanced visualization
- Capsular information regarding instability
- Superior assessment of complex tears
CT Imaging
CT provides specific advantages:
- Osseous detail superior to radiographs and MRI
- Acromion morphology and space assessment
- Acromioclavicular joint pathology precise evaluation
- Cortical bone involvement assessment
6. Treatment Options and Recovery
Conservative (Non-Surgical) Management
Phase 1: Acute Pain Management (Weeks 1-2)
- Rest and activity modification: Avoiding aggravating movements
- Ice application: 15-20 minutes several times daily
- Anti-inflammatory medications: NSAIDs (naproxen, ibuprofen) as tolerated
- Sling immobilization: Short-term use preventing excessive motion
Phase 2: Early Mobilization (Weeks 2-6)
- Pendulum exercises: Gravity-assisted shoulder mobilization
- Passive range of motion exercises: Gentle stretching within pain limits
- Supine internal and external rotation: Protected movement patterns
- Passive wall-supported stretches
Phase 3: Active Range of Motion (Weeks 6-12)
- Active-assisted exercises: Patient-initiated movement with therapist support
- Pulley exercises: Progressive mobility enhancement
- Scapular stabilization initiation: Gentle muscle activation
- Pain-guided progression: Honoring tissue healing response
Phase 4: Strengthening and Return to Function (Weeks 12+)
- Rotator cuff strengthening: Isolated muscle activation (resistance bands, light weights)
- Scapular stabilizer strengthening: Serratus anterior, lower trapezius, rhomboid emphasis
- Posterior chain strengthening: Back extensors and stabilizers
- Sport-specific or occupation-specific training: Progressive functional demands
Adjunctive Conservative Therapies
- Physical therapy: Evidence-based exercise programs (success rate 45-65% for small-medium tears)
- Corticosteroid injections: Subacromial or glenohumeral injections providing short-term pain relief (3-6 weeks typical duration)
- Platelet-rich plasma (PRP) injections: Emerging regenerative therapy showing promise (mixed evidence, facility dependent)
- Extracorporeal shock wave therapy (ESWT): Stimulating healing response (variable evidence quality)
- Manual therapy: Soft tissue mobilization, joint mobilization by qualified practitioners
Surgical Intervention
Surgical repair becomes necessary when:
- Conservative treatment fails after 3-6 months of compliant therapy
- Massive or acute tears with functional compromise
- Young, active individuals with significant functional demands
- Progressive neurological signs or functional deterioration
Surgical Approaches
- Arthroscopic repair: Minimally invasive, faster rehabilitation, excellent visualization
- Mini-open repair: Limited incision technique balancing visualization and soft tissue preservation
- Open repair: Traditional approach for complex tears, particularly massive repairs
Surgical Techniques
- Transosseous or transosseous-equivalent repairs: Restoring footprint contact
- Single-row repair: Reduced cost, faster rehabilitation
- Double-row repair: Superior healing rates, reduced re-tear risk (5-10% vs. 10-30% single-row)
- Suture bridge techniques: Biomechanically superior load distribution
Expected Outcomes Post-Surgery
- Pain relief: 85-90% of patients achieve significant improvement
- Functional improvement: 80-85% return to overhead activities
- Healing success: 80-95% depending on tear size, age, and technique
- Re-tear rate: 10-30% depending on tear characteristics and adherence
- Return to work: 3-6 months average
- Return to sport: 6-12 months average
7. Prevention Strategies for Cuff Health
Posture and Ergonomic Optimization
Workplace Ergonomics
- Monitor positioning: Eye level, arm’s length away, directly in front
- Desk height: Elbows at 90 degrees when seated
- Chair support: Maintaining neutral spine and scapular position
- Frequent breaks: Regular position changes every 30-45 minutes
- Keyboard and mouse positioning: Close to body, elbows at sides
Home Environment
- Sleeping position: Supporting affected shoulder with pillow
- Pillow height: Neutral cervical spine alignment
- Television viewing: Avoiding sustained overhead arm positioning
- Smartphone use: Keeping screen at eye level (preventing forward head posture)
Strengthening and Conditioning Programs
Rotator Cuff Exercises
- Side-lying external rotation (infraspinatus, teres minor)
- Prone external rotation at 90 degrees abduction
- Standing internal rotation with band resistance
- High-to-low band chop movements (diagonal patterns)
- Quadruped alternating arm/leg raises (dynamic stability)
Scapular Stabilization
- Prone shoulder packing (scapular retraction and depression)
- Push-up plus variations (serratus anterior emphasis)
- Rows and reverse flies (trapezius and rhomboid emphasis)
- Prone Y-T-W series (comprehensive scapular activation)
- Serratus anterior activation (wall and floor variations)
Comprehensive Shoulder Stability
- Planks and side planks with arm movements
- Quadruped patterns with contralateral limb movement
- Landmine press and lift patterns (functional movement integration)
- Cable and band rotational movements (multi-planar stability)
Flexibility and Mobility Work
- Posterior shoulder stretches (sleeper stretch, cross-body adduction)
- Doorway pectoral stretches (anterior shoulder capsule)
- Thoracic spine mobility (enhancing spinal extension and rotation)
- Posterior chain flexibility (hamstring, gastrocnemius, hip flexor)
Lifestyle Modifications
Smoking Cessation
Given smoking’s significant negative impact on tendon healing:
- Work with healthcare provider on cessation strategies
- Participate in smoking cessation programs
- Expect healing time improvement 6-12 months after cessation
Weight Management
- Maintain healthy BMI (18.5-24.9)
- Reduce inflammatory state from obesity
- Improve cardiovascular fitness for metabolic support
- Enhance functional capacity for activity tolerance
Activity Modification and Pacing
- Gradual progression: No sudden escalation in activity demands
- Warm-up protocols: 5-10 minutes of light activity before intense exercise
- Adequate recovery: Rest days between high-demand activities
- Cross-training: Varying movement patterns to avoid overuse
- Listen to body: Respecting pain signals as important feedback
Sleep Quality Optimization
- Sleep consistency: Regular sleep-wake schedule
- Adequate duration: 7-9 hours nightly for optimal recovery
- Supportive positioning: Pillow height and shoulder support
- Sleep environment: Cool, dark, quiet space
- Avoid pre-sleep stimulants: Caffeine, screens
8. When to Seek Medical Help
Red Flags Warranting Immediate Evaluation
Seek urgent medical attention if experiencing:
- Sudden severe pain with trauma or mechanism of injury
- Inability to move arm or complete functional loss
- Neurological symptoms: Numbness, tingling in specific dermatomes
- Systemic symptoms: Fever, chills, unexplained malaise
- Signs of infection: Heat, swelling, erythema
Indications for Specialist Consultation
Schedule evaluation with a sports medicine specialist or orthopedic surgeon when:
- Persistent symptoms despite 2-3 weeks of self-care measures
- Functional limitation affecting daily activities or work capacity
- Night pain interfering with sleep quality
- Weakness preventing normal movement patterns
- Failed conservative therapy after 6-12 weeks of appropriate management
- Occupational demands incompatible with injury severity
- Trauma mechanism concerning for significant structural damage
NBR Clinic—Your Trusted Sports Medicine Partner in Lahore
At NBR Clinic, Dr. Riaz Ahmed and the sports medicine team provide:
- Comprehensive evaluation using standardized clinical assessment and advanced imaging
- Personalized treatment planning based on individual factors and goals
- Evidence-based conservative management optimizing outcomes without surgery when possible
- Advanced surgical techniques for cases requiring operative intervention
- Rehabilitation coordination ensuring smooth return to function
- Follow-up care monitoring long-term outcomes and preventing recurrence
Dr. Riaz Ahmed’s expertise in sports medicine ensures that Lahore residents receive world-class care addressing their specific occupational and recreational demands.
9. Frequently Asked Questions (FAQs)
Q1: Can a rotator cuff tear heal on its own without surgery?
A: Small rotator cuff tears (less than 1 cm) may heal conservatively with proper rest and rehabilitation, with success rates of 45-65% for small-to-medium tears. However, larger tears typically require surgical repair for healing. Success depends on patient compliance with therapy, age, tear characteristics, and underlying tissue quality. Consult with Dr. Riaz Ahmed at NBR Clinic for individualized assessment and recommendations.
Q2: How long does recovery take after rotator cuff surgery?
A: Timeline varies based on tear severity and surgical technique:
- Initial recovery: 6-8 weeks with limited motion restrictions
- Early strengthening: 8-12 weeks with progressive activation
- Intermediate strengthening: 12-16 weeks with increased resistance
- Return to overhead activities: 4-6 months minimum
- Full functional return: 6-12 months
- Complete healing: Up to 12-24 months for tissue maturation
Individual factors (age, tear size, surgical technique, adherence) significantly influence timelines.
Q3: What exercises should I avoid with a cuff injury?
A: Generally avoid:
- Overhead pressing movements (military press, throwing)
- Wide-grip pull-ups or lat-pulldowns
- Dips (particularly weighted)
- Cross-body adduction beyond midline (internal rotation stress)
- Bench press with wide grip
- Downward dog (yoga) with full weight-bearing
- Heavy resistance early in recovery
Work with physical therapists at NBR Clinic for specific modifications based on your injury type and phase of recovery.
Q4: Is physical therapy necessary after rotator cuff surgery?
A: Yes, absolutely. Physical therapy is essential for:
- Preventing stiffness: Guided mobilization prevents adhesions
- Protecting repair: Progressive loading respects tissue healing
- Regaining function: Systematic strengthening restores capability
- Preventing recurrence: Motor control training reduces re-injury risk
Non-compliance with therapy significantly increases complications and reduces functional outcomes.
Q5: Can I return to overhead sports with a previous cuff injury?
A: Return to overhead sports depends on:
- Injury severity: Complete tears require more conservative return
- Time since injury/surgery: Adequate healing time is essential
- Rehabilitation completion: Full strength and motor control restoration
- Sport-specific demands: Some sports create higher demands than others
- Individual factors: Age, tissue quality, pain levels
Dr. Riaz Ahmed can provide specific recommendations based on sport demands and your individual recovery.
Q6: Are corticosteroid injections safe for shoulder pain?
A: Corticosteroid injections can provide short-term pain relief (typically 3-6 weeks) enabling more effective therapy participation. However:
- Limit frequency: Generally 3-4 injections annually to prevent complications
- Time-limited effect: Not curative, buying time for healing
- Potential risks: Tissue weakening with excessive use
- Individual variation: Some patients respond better than others
Use injections strategically as part of comprehensive management rather than sole treatment.
Q7: What is the difference between partial and full-thickness rotator cuff tears?
A:
Partial-Thickness Tears involve incomplete tendon damage:
- May affect articular surface (deep), bursal surface (superficial), or internal fibers
- Often less symptomatic than full-thickness tears
- May progress to full-thickness tears if untreated
- Conservative management more often successful
- Surgical repair indicated when conservative fails
Full-Thickness Tears involve complete tendon discontinuity:
- Typically more symptomatic with significant weakness
- Higher risk of progression if untreated
- Surgical repair generally recommended for functional demands
- More aggressive conservative treatment attempted in select cases
Imaging differentiates tear type and guides management decisions.
Q8: What is fatty infiltration and why is it important?
A: Fatty infiltration refers to fat replacing muscle tissue, visible on MRI and assessed using the Goutallier classification (grades 0-4):
- Grade 0-1: Minimal infiltration, excellent surgical prognosis
- Grade 2-3: Moderate infiltration, good prognosis but higher re-tear risk
- Grade 4: Severe infiltration, poor prognosis and challenging repair
Fatty infiltration develops over time with chronic rotator cuff tears and affects:
- Healing potential: Higher grades predict worse outcomes
- Repair feasibility: Severe cases may be irreparable
- Urgency: Advanced grade argues for earlier surgical intervention
- Prevention importance: Underscores need for timely diagnosis
Q9: Can poor posture cause rotator cuff injury?
A: Yes, postural dysfunction significantly increases cuff injury risk by:
- Reducing subacromial space: Forward posture narrows the space
- Altering biomechanics: Changing force distribution through structures
- Increasing impingement: Greater compression on tissues
- Reducing leverage: Weakening muscular advantage for function
- Creating compensation: Other muscles overwork
Posture improvement is fundamental to both treatment and prevention.
Q10: What distinguishes rotator cuff injury from cervical radiculopathy?
A:
Rotator Cuff Injury typically presents with:
- Lateral shoulder pain
- Pain worse with overhead/specific movements
- Weakness in specific motor patterns
- Preserved grip strength
- Normal neurological examination
- No paresthesias in specific dermatomes
Cervical Radiculopathy typically presents with:
- Lateral arm or hand pain following dermatome patterns
- Paresthesias/numbness in specific distribution
- Weakness following myotome patterns
- Neck pain accompanying arm symptoms
- Positive upper limb tension test
- Positive Spurling’s test
Clinical examination and imaging distinguish between conditions; Dr. Riaz Ahmed’s expertise ensures accurate diagnosis.
10. Conclusion: Expert Care at NBR Clinic, Lahore
Rotator cuff injuries remain among the most common shoulder problems affecting individuals across all age groups, particularly those with occupational overhead demands or athletic pursuits. Understanding the comprehensive spectrum of symptoms and risk factors enables early recognition and intervention, significantly improving long-term outcomes.
Key Takeaways
Symptoms to recognize:
- Shoulder pain, particularly worse at night
- Weakness with overhead activities
- Limited active range of motion
- Functional limitation affecting daily tasks
Risk factors to address:
- Age-related vulnerability
- Postural dysfunction and ergonomic issues
- Muscle imbalance and weakness
- Overhead or repetitive activity demands
- Lifestyle factors (smoking, sedentary behavior)
Prevention priorities:
- Postural optimization and ergonomic awareness
- Progressive strengthening programs
- Flexibility and mobility maintenance
- Activity pacing and recovery emphasis
- Lifestyle modifications supporting healing
Management approach:
- Early recognition and medical evaluation
- Evidence-based conservative management
- Surgical intervention when indicated
- Comprehensive rehabilitation
- Long-term follow-up and prevention
Why Choose NBR Clinic for Your Shoulder Care
Dr. Riaz Ahmed and the sports medicine team at NBR Clinic in Lahore provide:
- Expert diagnosis: Utilizing comprehensive clinical examination and advanced imaging
- Personalized treatment: Tailored management based on individual factors, goals, and demands
- Conservative expertise: Maximizing outcomes without surgery when possible
- Surgical excellence: Advanced techniques for cases requiring operative intervention
- Rehabilitation coordination: Ensuring smooth recovery and return to function
- Lahore-centered care: Understanding regional occupational and recreational demands
- Ongoing support: Long-term follow-up and prevention strategies
For Lahore residents experiencing shoulder symptoms, don’t accept functional limitation. Contact NBR Clinic today to schedule an evaluation with Dr. Riaz Ahmed and take the first step toward recovery.
Professional Credentials and Expertise
Dr. Riaz Ahmed brings specialized expertise in sports medicine and orthopedic care to NBR Clinic, with particular emphasis on shoulder injuries affecting Lahore’s active population. His comprehensive approach combines evidence-based medicine with individualized patient care.
Final Recommendations
- Recognize early symptoms: Don’t ignore persistent shoulder pain or weakness
- Seek timely evaluation: Early diagnosis improves treatment options and outcomes
- Commit to prevention: Posture, strengthening, and activity modification prevent recurrence
- Trust expert guidance: Work with qualified specialists like Dr. Riaz Ahmed for optimal care
- Embrace rehabilitation: Compliance with therapy determines long-term success
Your shoulder health directly impacts quality of life, occupational function, and recreational enjoyment. Invest in proper care and prevention today to maintain long-term shoulder function and wellbeing.